

What is posterior impingement?
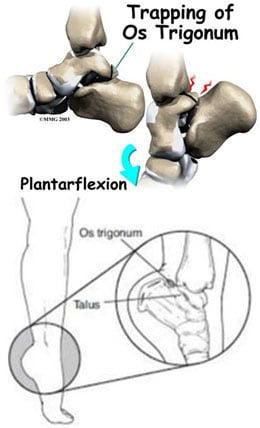
Posterior ankle impingement syndrome causes pain in the back of ankle. It typically occurs in a position of forced plantar flexion (foot pointing downwards). Push-off maneuvers, particularly with the ankle in plantarflexion, are typical of this disorder, as well as increased pain going down stairs. This occurs with less frequency than other ankle conditions, and thus there is often a delay to diagnosis and treatment, especially when the first doctor you see is to a doctor other than a foot and ankle orthopedic surgeon who is aware of the condition.
Causes
Pain might also occur if the flexor hallucis longus (FHL) tendon gets irritated. This can happen if the tendon doesn’t fit well because the tunnel is too tight or the tendon is too big, or if the tendon is inflamed and swollen (called tenosynovitis).
An ankle sprain may also cause a tear of the posterior ankle ligaments. The torn pieces can flip inside the joint. They can get pinched between the joint surfaces and cause pain. This problem is called posterior soft tissue impingement.
Posterior impingement syndrome can be triggered by an injury, such as an ankle sprain, or can occur chronically with activities or sports that frequently cause the downward pointing of the toes, such as ballet and gymnastics. The os trigonum or soft tissue can get squeezed between the ankle and heel bone.
Diagnosis

Posterior impingement syndrome can mimic other conditions such as an Achilles tendon injury, ankle sprain, or talus (ankle bone) fracture. Diagnosis begins with questions from your surgeon about the development of the symptoms and a thorough physical examination. X-rays are ordered to evaluate any bony abnormalities.
An MRI is utilized in certain instances to evaluate the soft tissue around the ankle as well as the ankle and subtalar joint. This imaging is to determine how far back in the ankle the problem goes as well as determine surgical planning should surgery be warranted.
Nonsurgical treatment
Relief of the symptoms is often achieved through treatments that can include a combination of the following:
- Rest. Limit the amount you are on the injured foot/ankle.
- Immobilization. A walking boot may be used to keep the foot and ankle from moving and allow the injury to heal.
- Ice. Apply an ice pack to the injured area, placing a thin towel between the ice and the skin.
- Compression. An elastic wrap may be recommended by your surgeon to control swelling.
- Elevation. The ankle should be raised slightly above the level of your heart to reduce swelling.
- Physical therapy. Your surgeon may start you on a rehabilitation program to help with the pain and to assist in function and strengthening.
- Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), may be recommended to reduce pain and inflammation. In some cases, prescription pain medications are needed to provide adequate relief.
- Injections. Sometimes cortisone and local anesthetic are injected into the area to reduce the inflammation and pain.
Surgery
Symptoms usually improve with non-surgical treatment. However, in some patients, surgery may be required to relieve the symptoms. Surgery typically involves removal of the scar or inflammatory tissue, and os trigonum if present, as this extra bone is not necessary for normal foot function. This now can be accomplished with a minimally invasive posterior arthroscopic technique.
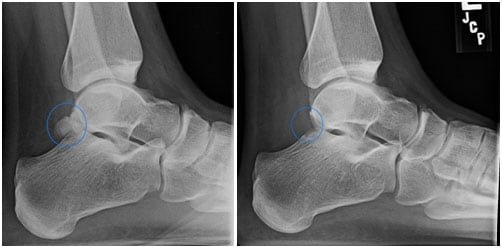
Left Figure: X-ray before the operation showing abnormal bone prominence
Right Figure: X-ray after the operation showing removal of the abnormal bony prominence after a surgery that used the minimally invasive endoscopic approach with two 1cm long incisions.
Arthroscopy is a surgical procedure in which the inside of a joint, such as the foot, is examined and treated using a camera and instrumentation that are inserted through small incisions typically one centimeter in length (called portals). Two small portals are typically used to perform the procedure.
Compared to traditional open incisions, the advantages of arthroscopy include:
- Earlier rehabilitation;
- Accelerated rehabilitation course;
- Less pain and blood loss;
- Lower rate of infection.
After surgery a splint or boot will be placed on the foot/ankle you had surgery on. You don’t put weight on the foot/ankle that was operated on until your surgeon tells you that you are allowed to. It usually takes eight to 12 weeks for athletes to return to play after posterior ankle arthroscopy and os trigonum excision, but this time certainly can vary.
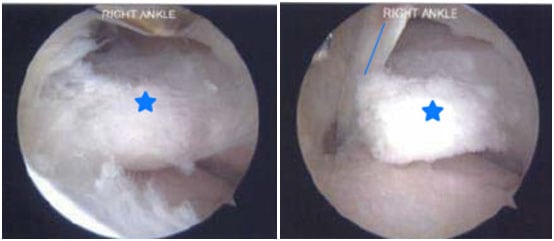
Figure 2A. Endoscopic picture of elongated posterior process of the talus (delineated by the star) in active gymnast/cheerleader with posterior ankle pain.
Figure 2B. Endoscopic picture of elongated posterior process of the talus (star) and the flexor hallucis longus tendon (blue line) adjacent to it.
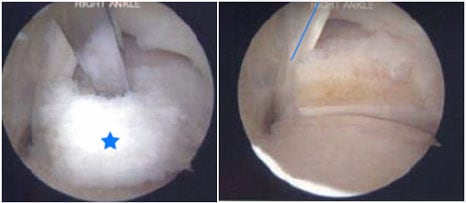
Figure 2C. Endoscopic picture of removal of painful elongated posterior process of talus (star). Metal osteotome used to remove.
Figure 2D. Endoscopic picture after removal of painful elongated posterior process of talus.