What is Hip Femoroacetabular Impingement?
Femoroacetabular impingement of the hip is a disorder where there is abnormal contact between the femoral head/neck (the “ball”) and the acetabular rim (the “socket”). Essentially, when a patient rotates his/her hip, the “ball” and “socket” bump together.
Patients with femoroacetabular impingement have a natural hip anatomy that predisposes to this condition. When coupled with repetitive rotational activities of the hip the result can be symptomatic impingement and hip pain.
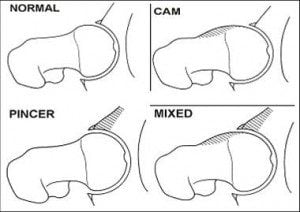
Diagramatic representation of FAI. Cam type impingement is caused by abnormal bone formation about the femoral head. Pincer type impingement is caused by over coverage or rotation of the acetabular wall. Mixed type is a combination of the two
What Are the Symptoms of FAI?
Patients with symptomatic femoroacetabular impingement often describe pain deep within the groin or lateral aspect of the hip. Pain is often exacerbated by hip rotation; most commonly internal rotation of the hip. Patients can also have a feeling of catching or locking in the hip. Getting in and out of a car, squatting, running and prolonged sitting can all lead to increased symptoms. Left untreated, it is felt that femoroacetabular impingement may be one of the causes of early onset osteoarthritis of the hip.

38 yo male with Cam type femoroacetabular impingement of the left hip. Patient has significant groin and lateral hip pain with running and also with prolonged periods of driving. Note the bony buttressing about the lateral aspect of the femoral head and neck
Femoroacetabular impingement can occur in one of two ways. The first type of impingement is CAM impingement. In this condition, there is a raised area of bone on the femoral neck which impinges on the wall of the acetabulum when the hip is rotated. Over time, this “bump”of bone can cause damage to the labrum and cartilage surface of the acetabulum.
In the second type of impingement, there is excess coverage of acetabular bone which can lead to abutment of the lip of the cup on the neck of the femur. This is called PINCER impingement and can also lead to damage of the labrum and cartilage. Some patients can have a combination of both CAM and PINCER impingement.
Minimally-Invasive Treatment of Femoroacetabular Impingement
Femoroacetabular impingement is amenable to arthroscopic surgical treatment. Hip arthroscopy for the treatment of impingement is one of the most common hip procedures performed by Dr. Wind. Treatment is guided by the type of impingement present. Diagnostic imaging procedures often obtained include magnetic resonance arthrograms (MRA) and 3-dimensionally reconstructed CT scans. The studies are useful in identifying labrum tear and cartilage damage. The images are also helpful in identifying the impinging bony structures that must be removed during surgery.

Image of 3D CT reconstruction of the pelvis. This study is used to help identify areas of Cam or Pincer impingement that must be removed during surgery. On this study note the bony buttressing of the Cam lesion on the femoral neck

Arthroscopic femoral neck osteoplasty. The cam lesion (bony bump) along the femoral neck has been removed arthroscopically thereby relieving the impingement of the hip
During arthroscopic surgery, labral tears can be treated with debridement or repair. Cartilage damage can also be treated. Impinging bony structures, whether on the cup or on the femoral neck, can be corrected by removal of the impinging bone. Removal of this bone is described as a “femoral neck osteoplasty” or an “acetabular osteoplasty.” After surgery patients are started in an aggressive and focused physical therapy program.